Browse: Home / Professionals
By dr on January 10, 2025
This past September I took NeuroKinetic Therapy (NKT) Level One with Kathy Dooley at Catalyst S.P.O.R.T. NYC. Several of my friends have taken this course and highly recommended it. My philosophy is that knowing more information, having more tricks up your sleeve, and learning new perspectives can only help your patients.
This review is simply my interpretation of the NKT system and how I have tried to incorporate it into my practice. I do not work for NKT or represent NKT. Please visit the NKT website for the authoritative description of the approach.
Kathy Dooley
I want whatever Kathy Dooley has in the morning. She has an insane amount of energy, is extremely knowledgeable, and was very animated during the entire course. She not only has a deep understanding of the NKT approach, but she has mastered it clinically. For me, the best part of the course was watching Kathy perform live demonstrations. These not only displayed the NKT technique, but allowed for a greater understanding of how to incorporate the approach into daily use. She gave a clear, clinical perspective of how she chooses which muscle to “Therapy Localize” and how to incorporate the results of the assessment into your patient’s care.
My favorite Kathy quote:
“I’m not busy because I’m good. I’m busy because I empower my patients.”
Quick Definitions & Semantics
Throughout the course there seemed to be some confusion over some terms and semantics. Hopefully this will help clear things up and make it less confusing.
Here is an oversimplification of the common terms used in the NKT approach:
- Facilitated = On = Strong = Muscle Firing = Neural Drive = Efferent Motor Outflow
- Inhibited = Off = Weak = Muscle Not Firing = No/Minimal Neural Drive
Try not to associate these terms with good or bad. In certain situations you want muscles inhibited. In certain situations you want muscles facilitated. But in this NKT system, you do not want to find a muscle that is so inhibited that it can’t even match a light force. This doesn’t mean inhibition is a bad thing, it just means that muscles should be able to go from an inhibited state to a facilitated state when called upon.
What is NKT?
- “NeuroKinetic Therapy (NKT) is an application of motor control theory, neuroscience, and functional anatomy (neurobiomechanics) that will help you unravel the cause of faulty movement patterns in the brain’s motor control center.” -David Weinstock
NKT gives you another lens through which to view your patients. It uses an innovative manual muscle test coupled with a trial and error of inputs with the goal of improving neural drive.
Here’s the basic progression:
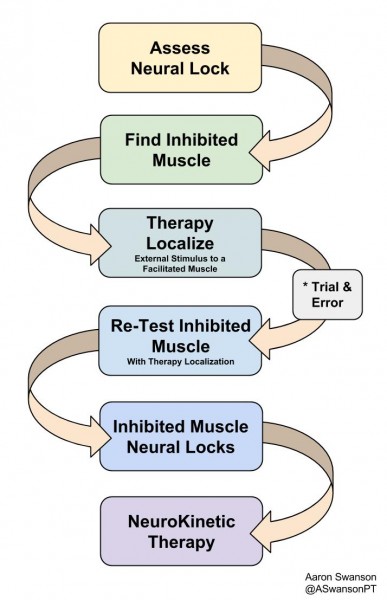
NeuroKinetic Therapy
The main goal is to find a muscle that does not have a Neural Lock. A muscle that can’t even meet a light resistance (inhibited).
The next step is to find a facilitated muscle (a muscle that is already on) to Therapy Localize. Therapy Localization is just when you apply an external input to a “facilitated” muscle while re-assessing the inhibited muscle. It’s simply adding input to change the output, but it’s assessed instantaneously.
Which “facilitated” muscle you pick first to Therapy Localize depends on many factors. It depends on their history, the mechanism of injury or dysfunction, their posture, their breathing pattern, their SFMA breakout, their PRI pattern, their whatever. There are many ways to get to the same place.
The magic happens when you find a “facilitated” muscle that when you Therapy Localize, it turns the inhibited muscle on. Once you find this, you have an input to output response that you can use for the rest of your assessment and treatment. You have a specific muscle to “release” that will faciliate another muscle that needs more neural drive.
After you find this connection the treatment is wide open. You can incorporate a self-release in a circuit. Example: “inhibited” glute max (no neural lock), “facilitated” rectus femoris. Therapy Localization of the rectus femoris results in improved glute max neural drive (neural lock). An example circuit: foam roll rectus femoris, single leg hip thruster, RKC plank, single leg deadlift, repeat (including foam roll at every set). This is just an example – the options depend on your creativity.
This may sound very confusing. But in clinical practice and watching a live demonstration, it becomes much clearer and easier to use.
3 Things I Learned From NKT
1) A New Manual Muscle Test
Traditionally we use manual muscle testing that determines a “specific muscles strength”. However, this doesn’t take into consideration of the complexity of the nervous system. It doesn’t take into consideration the complexity of proximal stability. It doesn’t take into consideration the global system. It doesn’t give you that much information – it tells you if the body can match the random resistance applied from the tester.
In it’s simplest form, NKT is a way to assess the specific neural drive of the musculoskeletal system. It looks at how the nervous system interacts with specific movement patterns. It gives you a specific force, at a specific location, with a specific outcome that relates to the rest of the body.

This is how some people are currently manually muscle testing the biceps
2) The Importance of a Neural Lock

It’s a light touch and the should only meet your pressure, not exceed it (picture idea from Ming Ming Su-Brown)
The overall theme is the same as what some strength and conditioning coaches preach – “you can’t strengthen a muscle that you can’t activate”. In this sense, you are simply looking to see if the muscle is ON (facilitated) or OFF (inhibited). There are graded levels of resistance to assess strength, but the innovation lies in the light touch assessment of the nervous system.
This light touch assessment is simply checking for what they call a “Neural Lock”. It’s the lightest manual muscle test you’ve ever done. You’re simply putting a light force on the body to see if it can “facilitate” the necessary muscles to match the resistance. You’re checking to see if the brain can tell the specific “muscles” to turn on (facilitatie). You’re checking the motor neurons ability to fire from the CNS. You’re not checking strength – you’re checking availability.
An important factor here is that the patient must only “meet your resistance”. I’ve noticed that many go into a high-threshold strategy and over fire all the synergistic muscles to try to make up for the “inhibited” muscle. The light touch shouldn’t be met with a life or death response.
3) A Manual Therapy Assessment
After our manual interventions we often re-assess many different outputs. We assess:
- Pain (depends on an immeasurable amount of variables)
- “How it Feels” (depends on an immeasurable amount of variables)
- Global Movement (depends on many variables)
- Isolated ROM (few variables involved)

How is George going to know what’s really happening if he’s not assessed after the manual technique?
The more variables involved in an output, the more complicated the relationship. This is why re-assessing pain or how it feels may not be the most accurate assessment of your manual skills. It may be more of an assessment of the patients beliefs of your manual skills or your ability to prime the patient, but that’s another story.
Re-assessing a simple input-output relationship, like ROM, gives the practitioner a more accurate way to assess the manual-output relationship.
NKT suggests another simple input-output relationship we should assess – muscle strength/activation. Simply perform manual therapy to “release” a muscle, then re-test a specific muscles strength. You have nothing to lose and specific strength to gain.
For the Critics
I know there are many skeptics out there who will scoff at many of the NKT concepts. I just want to address them here first. If I can turn one pessimistic troll into an inquisitive thinker, then I will consider this a success.
Isolated Muscle Testing
We all know there is no way to truly isolate a muscle without a surgical scalpel. And I’m sure the NKT guys agree. But it’s much easier to say it’s the quadratus lumborium test than the supine lateral flexion with resistance at the ankle test. The specific muscle tests are more about the intention. It’s not meant to disregard to complexity of the connective tissue/fascia system or the nervous system.

Once it hits your lips…
For the global movement people that have a difficult time with non-functional assessments, just consider this as a more specific movement pattern. It’s throwing a load into a system and checking the output. There’s less variables involved with a muscle test compared a complex global movement. This means the outputs measured will be more specific to the chosen inputs. It’s further down the funnel.
If you ask someone to squat (global movement assessment) and their knee caves in it could be a million different things. Specific NKT muscle testing is one of many things you could do that could help you narrow the infinite. It gives more information to help answer the bigger questions.
Facilitated/Inhibiting
We all know muscles are not just off or on. We know we’re not going from full paralysis to full tetany throughout a gait cycle. That said, there is a constant wave of neural drive to assist with movement patterns. We know that some muscles decrease their neural drive and some increase it to accomplish a task. This is a very complex interaction of the body, the environment, and the task.
What NKT does is try to offer a snapshot of a specific area under reproducible constraints. It helps display the variability of a specific, reproducable motor program. It helps narrow the infinit.
Unless you’re Bernie, you don’t have any muscles that are truly off.
Magic
We all know there’s no such thing as magic. But many movement professionals have experienced a drastic change in output from a minimal change in input. Most of the time this chalks up to a temporary neurological response. This temporary neurological response is perceived as magic to people who don’t understand the human body or the nervous system (most of your patients).
Most professionals know this “magic” is not long lasting. It will take many frequent inputs to get it to stick. But for the anxious patient who doesn’t yet buy in to what you’re doing – this is profound. They feel the difference immediately. They don’t have to wait 3-6 weeks to start seeing changes. They don’t have to depend on your manual therapy. They don’t have to change their beliefs. They are given hope. They get excited. Then they buy in and believe everything else you say. Regional interdependence, pain science, and the bodies natural asymmetries are much easier to talk about when the patient already trusts you.
Overall
I enjoyed the NKT class and was happy to learn a new perspective on muscle testing. I have been able to incorporate it into my practice very easily. Similar to the SFMA, the NKT does not remove anything from your practice. It just adds another assessment for more information. You’ll never find what you’re not looking for
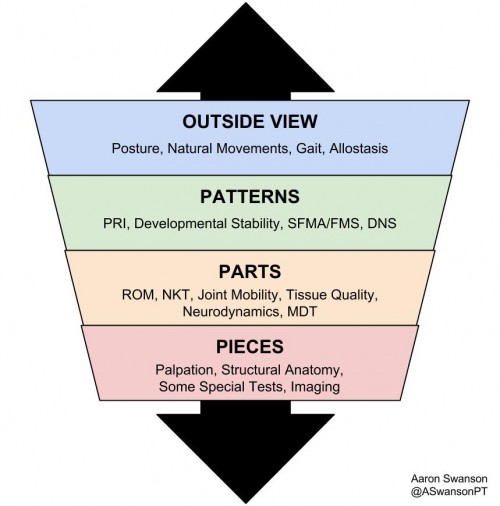
My funnel now and my funnel in college are very different
Posted in Professionals | Tagged assessment, Review |
By dr on March 24, 2018
Posted in Patients, Professionals |
By dr on April 4, 2017
Click here for this edition’s table of contents
Lower Extremity
Hip
1) The glutes are internal rotators too…
2) Some great clinical insight on chronic hip flexor strains from Dave Tilly. I love the idea of treating the hip like the shoulder in regards to PNF rhythmic stabilization and wall ball circles.
3) The hip and the back are always related. “The authors concluded that dynamic pelvic orientation significantly influences the functional orientation of the acetabulum. This study also found that people with impingement have reduced trunk control bilaterally, supporting the need to include trunk rehabilitation in treatment. This has implications for therapists rehabilitating patients with symptomatic FAI as not only should the trunk be a strong focus of rehabilitation but pelvic positioning during exercise and ADLS can have an impact on the positioning of the hip and range of movement.” Continue reading “2017 Hits : Vol. 1 : Clinical Lower Extremity”
Posted in Professionals | Tagged The Hits |
By dr on March 31, 2017
Click here for this edition’s Table of Contents
Upper Extremity
Shoulder
1) Too many people advance too quickly with pull up progressions. Too few spend enough time mastering the hang. Dan Pope writes a nice concise post with 3 basic hang exercises for the shoulders. And he backs it up with some solid biomechanical logic.
2) Eric Cressey gives a nice 3 minute breakdown of proper cueing for the scaption exercise. I think a tactile cue for posterior tilting the scapula is one of the best rehab interventions out there.
3) Heart disease and rotator cuff symptoms are linked in a new study. Maybe it has to do with circulation? Or maybe the rotator cuff symptoms are just the output of a lifestyle dysfunction?
4) Erson shares a nice example of a motor control shoulder dysfunction. Before you jump to conclusions, assess their movement impairment with different patterns (i.e. posture changes, sequencing, distal positioning, centration, etc.). Continue reading “2017 Hits : Vol. 1 : Clinical Upper Extremity”
Posted in Professionals | Tagged The Hits |
By dr on March 18, 2017
Table of Contents
Miscellaneous
- “The patient’s nervous system can sense both a lack of practitioner confidence, as well as a lack of control.” -Dr. Andrei Spina (via Shante)
1. “Evidence has shown that performance and variability have an inverse curve relation (too little variability, performance suffers and with too much variability, performance also suffers). Current evidence shows that an optimum balance of variability seems to be the key to maximize performance of an individual and achieving this balance is key in recovery.” –Adriaan Louw
2. Assessing gait is a skill we should always continue to develop. Even on the blink level it provides useful information. “Walk speed = “vital sign”. Connects to fall risk, dependency, & hospital. Community design & PA programs matter”
3. This might explain why marathon runners often stumble into our clinic a month before their race. “Overtrained athletes have abnormal inflammatory and anabolic responses to exercise, indicating that their body is not responding to exercise the way that it should.” Continue reading “2017 Hits : Vol. 1 : Clinical”
Posted in Professionals | Tagged The Hits |
By dr on December 4, 2016
Click here for this edition’s Table of Contents
1) Everyone is different (joint, osseous structures, myofascial structures, developmental history, etc.). So it’s easy to understand why “there are no systematic advantages of one foot strike pattern over another when it comes to running economy”. #DynamicSystem
2) “Proximal joints act as motors and distal joints as adjustable dampers & springs” -Derek Griffin
3) Are we overlooking the blood flow component of tendinopathies? “Tendon blood flow tends to decrease with age and compression, which often results from increased mechanical load. This decreased vascularization, at least theoretically, can contribute to the probability of tissue damage as tissue compliance and flexibility will be compromised (LER). Oxygen consumption of ligaments and tendons is 7.5% lower than skeletal muscle, which may contribute to longer healing times (2,3).”
4) The Gait Guy’s breakdown of a case study is always worth the time. In this one they find the driver in the spine. In this one they breakdown the biomechanics of 4 different runners.
5) What do we use to regulate ourselves? Thought or awareness? Seth teaches us how using thought can lead to chronic pain. “But we can’t think our way out of a physical “problem”. The autobiographical self (story we tell ourselves) and the embodied self (our experience in the present moment) are separate neural networks.“ Continue reading “Fall Hits 2016: Clinical”
Posted in Professionals | Tagged The Hits |
By dr on December 4, 2016
This is a collection of information to help improve health and movement. It includes articles, videos, and quotes that I have found helpful in studying the human species. Due to the complexity of this subject matter, I have tried to include a variety of variables that can influence the dynamic system.
In an attempt to avoid information overload, I’ve separated the information into different categories.
I will post each category separately to make it easier to scroll through.
The links below will be added over the next month as they are posted.
Feel free to follow me on social media to keep up to date on the latest postings.
Twitter
Instagram
Facebook
YouTube
AG Project Blog
Making this information accessible for everyone takes a great deal of effort and time. If you have the resources, please consider a donation. Your support to maintain this website is greatly appreciated.
Table of Contents
Blood flow, self-regulation, studies, headaches and furrowing, hip flexor strength, forward lunge trunk angle, running fatigued, Kathy Dooley anatomy, best breathing gifs of all time
How knee pain will end your life (another reason why PT is important), decline of american health, and why you should worry about your significant other’s health
What kind of narrative are you living?, emotion states are all there is, bad feelings=irrational beliefs, pain is in the body too, Dr. Sarno, why we need diagnoses, and opiods
Work on yourself to work on others
volume effect, split squat lunge torso angle and feet distance, vertical quadruped
Motivation and stuff
Microbiome and stuff
Trees, titles, and rhinos
Subscribe below for the latest updates
We don’t share your email address. It’s just for updates on when the good stuff comes out.
Posted in Professionals |
By dr on June 24, 2016
The Hits
This is a collection of some of my favorite articles from the past month. I bolded and underlined the numbers of the articles that I found most remarkable. Of course, this is just my bias. I think all the articles here have value. I realize that some readers may be looking for something more brief.
Unfortunately, I am currently busy with a couple other projects and do not have the resources to produce a collection of “Hits” every month. However, I’ll continue to do my best to get it out as frequently as I can.
For a more real-time update of movement and health information follow me on social media:
Instagram – exercise pictures, movement flows, and Rigby
Facebook – movement and health articles (geared towards the public to improve education)
Twitter – weird abstract comments, out of context stuff, quotes, and good stuff from things I’m reading
If you enjoy this collection and find it valuable, please share it with other professionals. If you have the resources available, please make a donation to help me run this site and continue to put information out there to help movement professionals grow.
Also, I want to encourage any readers to share their favorite articles, books, or podcasts of the month in the comments below. I know there’s a ton of great stuff out there that isn’t on my radar. It will introduce me and other readers to new perspectives.
Clinical
- “You can recognize a deep truth by the feature that it’s opposite is also a deep truth” – Frank Wilczek
1) “The human body is one of the most complex organizations of matter in the known universe. To understand it, we must build models, use metaphors, and deal in abstractions. This necessarily involves ignoring certain details, creating simplified pictures, and relying on metaphors that have the potential to mislead. But we have no choice! Models and metaphors are indispensable thinking tools to understanding the body. Each model is a different perspective from which to see the world, with its own unique insights and blindspots.” –Todd Hargrove
2) Michael Mullin shares his highlights and thoughts from a great article on the diaphragm.
3) Solid article from Chris Beardsley – “Eccentric training produces specific gains in eccentric strength, partly by increasing the strength of the passive elements in a muscle, which makes them stiffer. This gives muscles a greater capacity to decelerate, and absorb energy. This superior ability to absorb energy is probably why eccentric training then leads to a reduction in the risk of getting a muscle strain injury.”
4) “If existing interventions don’t adequately address the way patients use somatosensory versus visual information, that could explain why patients with CAI often continue to experience episodes of ankle sprain or giving way despite having gone through a full balance training protocol.” Continue reading “May-June Hits 2016 : Tom Myers, Self-Image, Pain & Noses, Instagram, Diet & Tendons”
Posted in Professionals | Tagged The Hits |
By dr on April 14, 2016
The Hits
This is just a collection of some of my favorite articles from the past month. I bolded the numbers of the articles that I found most remarkable. Of course, this is just my bias. I think all the articles here have value. I just realize that some readers may be looking for something more brief.
Also, I want to encourage any reader to share their favorite articles, books, or podcasts of the month in the comments below. There’s only so much information that I can go through in a month. I know there’s a ton of great stuff out there that isn’t on my radar. It will not only help introduce me to new perspectives, but it will provide other readers this opportunity as well.
Epistemological Arrogance
1) “Epistemic Arrogance: measure the difference between what someone actually knows and how much he thinks he knows. An excess will imply arrogance, a deficit in humility. An epistemocrat is someone of epistemic humility, who holds his own knowledge in greatest suspicion.” -Nassim Nicholas Taleb
2) Complex does not mean complicated – “Complicated systems are usually built from design, and include cars, computers and buildings. Complex systems were not built but evolved, and include living things, ecologies and economic systems.” Great piece by Todd Hargrove
3) Sometimes in the buffet style of information digestion that is the internet, there will be “gurus” out there who will claim “all health problems can be fixed with these “3 things you’re not doing”. Or worse, they’ll take a “if your not doing ___ you’re missing the boat” approach.
Those of us in clinical practice know it’s not this simple. The problem is that ranting about a simple, secret solution to a complex problem gives people either false hope or it makes them feel bad as a clinician that they don’t know about the “secret answer”. And I don’t think anyone in healthcare should be making clinicians feel bad or teaching through narcissistic ways.
My intention with this article is simply to put something out as a clinician that says it’s not simple. There are no easy answers when it comes to treating the human species. Each patient will be complex. It’s a very intricate system with many parts. It doesn’t work out all the time. Some people don’t get better. Sometimes they need a different approach or control parameter. Continue reading “April Hits 2016 : Epistemological Arrogance, State of Healthcare, Cognitive Bias, Arm Ergometer, Insulin/Glycemic Index, Nutrient Timing, Reform the World”
Posted in Professionals | Tagged The Hits |
By dr on April 4, 2016
- “For every complex problem there is an answer that is clear, simple, and wrong” -H.L. Menken
Keeping “it” simple is important at times. It prevents us from becoming overwhelmed, clarifies concepts, aids in general understanding, and directs the focus towards a single goal. Most importantly, keeping it simple is necessary when communicating new topics or concepts to others. However, the problem occurs when keeping it simple is used a substitute for understanding the complexity. Continue reading “Embracing Complexity: The Mountain Stream Metaphor”
Posted in Patients, Professionals | Tagged assessment, Lumbar |
By dr on March 15, 2016
The Hits
This is just a collection of some of my favorite articles from the past month. I bolded the numbers of the articles that I found most remarkable. Of course, this is just my bias. I think all the articles here have value. I just realize that some readers may be looking for something more brief.
Also, I want to encourage any reader to share their favorite articles, books, or podcasts of the month in the comments below. There’s only so much information that I can go through in a month. I know there’s a ton of great stuff out there that isn’t on my radar. It will not only help introduce me to new perspectives, but it will provide other readers this opportunity as well.
Phone Addiction
- “Only one thing made him happy and now that it was gone everything made him happy.” -Leonard Cohen
A big part of our ability to live longer comes from the knowledge of what harms us. Smoking, aluminum production, lead, high fructose corn syrup, artificial sweeteners, poor sleep, sitting, and now smartphones.
Unfortunately, not many people are open to the idea that their cell phones are bad for them. At least not beyond a surface level acknowledgement.
I wrote this article on 25 reasons why your cell phone is bad for you. It has a ton of resources for many different categories. Hopefully it will serve as a resource to bring awareness of the hazards of smartphone overuse. Share it with those that you think need to hear it.
Here’s a similar article with detailed recommendations on how to “Break Your Smartphone Addiction” Continue reading “March Hits (2016)”
Posted in Professionals | Tagged The Hits |
By dr on February 24, 2016
- “Men have become the tools of their tools.” -Henry David Thoreau
Before I proceed and alienate everyone, I first want to clarify that I am not against technology and I don’t think smartphones are inherently bad. I’m not trying to pull a John Connor and convince you to rage against the machine and destroy your cell phone.
In fact, I think technology is a critical component of our culture’s development. Smartphones can be extremely helpful. Not only can they end many arguments with instant fact-checking, but they provide an endless supply of free information and the ability to connect with almost anyone in a first world country. This creates many opportunities that wouldn’t exist otherwise.
But like my mom always says, “everything is okay…in moderation.”
The problem arises when smartphones go from a tool to a behavior. Soon after this, addiction ensues. Next thing you know you’re so dependent on your cell phone that you’re looking for outlets in public places. Continue reading “The Problem with Smartphones”
Posted in Patients, Professionals | Tagged Prevention / Recovery |
By dr on February 15, 2016
The Hits
This is just a collection of some of my favorite articles from the past month. The bolded the numbers of the articles that I found most remarkable. Of course, this is just my bias. I think all the articles here have value. However, I realize that some readers may be looking for something more brief.
Also, I want to encourage any reader to share their favorite articles, books, or podcasts of the month in the comments below. There’s only so much information that I can go through in a month. I know there’s a ton of great stuff out there that isn’t on my radar. It will not only help introduce me to new perspectives, but it will provide other readers this opportunity as well.
Clinical
- “The job of a skilled therapist is to detect where the system is open to change, to provide the appropriate new input to destabilize the old pattern, and to facilitate the person’s seeking of new solutions” -Esther Thelen (via Seth Oberst)
1) One of the better ACL articles I’ve read in a while. Read this post – especially the part on terminal knee flexion. Great explanations and quick video demonstrations. Very useful for the clinic tomorrow. Here’s one gem from the article series – “The ability of the hamstring to pull the heel to butt is a necessary pre-requisite for dorsiflexion.”
2) The Longus Capitus attaches to the foramen magnum? How did I overlook that?
3) Sick of patients asking for you to put their pelvis/SIJ back in place? Try these 3 steps to change their thought virus.
Challenge a Concept
Provide an Alternative Concept
Provide Evidence for a New Concept Continue reading “February Hits (2016)”
Posted in Professionals | Tagged The Hits |
By dr on February 11, 2016
Guest Post: Biomechanical vs. Anatomical Breathing
By Cameron Yuen
This post was inspired by a discussion I had with Aaron about the StrongFirst snatch test. This test, which basically involves snatching a 24kg kettlebell 100 times within 5 minutes, is well known for it’s ability to leave even the most conditioned athletes gasping for air. Continue reading “Guest Post: Biomechanical vs. Anatomical Breathing”
Posted in Patients, Professionals | Tagged Biomechanics, Breathing |
By dr on January 5, 2016
News
As you may or may not have read in a previous article, I’m leaving NYC and moving to Asheville, NC. My girlfriend and I have decided to take advantage of this transition and are taking a small “sabbatical”. Part of this time off involves a selfish 3 week trip to New Zealand this month. Unfortunately, this means I won’t be able to get a “January Hits” post out this month. I do have posts scheduled on my Facebook account, but other than that you guys are on your own! Continue reading “The Best of 2015”
Posted in Professionals | Tagged The Hits |
By dr on December 16, 2015
News
Unfortunately, my time in NYC is coming to an end. I’ve spent over 8 years here and I’ve enjoyed the buzz, the people, the music, and the late night slices . However, I’m ready for a lower cost of living, a little less concrete, a little more nature, and a slower pace. So I’m moving to Asheville, North Carolina in January.
I wrote this article on 5 things I’ve learned from my mentorship at Dynamic Sports Physical Therapy. I feel that one thing missing from the movement social media world is a discussion on the things that happen “behind the scenes” that make the difference between a good clinician and a great one. While evidence, trendy semantics, cool neuro language, the latest performance enhancement, and arguments over what someone else is doing can be fun to read, they don’t always translate to improving clinical performance.
If there’s anything I’ve learned from my 5 years as a PT in NYC, it’s that there’s a lot more to treating patients than what you can read in a journal, book, or blog. Hopefully the article above will help explain this concept (yes, I know it’s a blog and I’ve just contradicted myself, but if you read it you’ll get the point). Continue reading “December Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on December 7, 2015
I was very lucky to be mentored by Chris Johnson after PT school. I observed and worked part-time in his clinic for almost a year. I learned a tremendous amount from him and was excited to get an update on his approach during his Treadmill Analysis Workshop this past Wednesday.
Chris is the premier running expert. He doesn’t practice what he preaches, he’s a master of it (2x Kona Qualifier). He dives deep into research to stay current on the latest evidence and to improve care. And most importantly, he spends a ton of time treating and training endurance athletes.
Needless to say, he has some valuable information to share. Continue reading “Course Review: Chris Johnson Treadmill Analysis Workshop”
Posted in Patients, Professionals |
By dr on December 1, 2015
The minimal effective dose rule goes into effect here. You want to achieve the necessary movement change with the minimal amount of sensory change. If you throw too many different cues (verbal, visual, proprioceptive) at the same time, it will clog up the system and wear down the patient. As mentioned in the previous articles, it comes down to attention economy – you always want the movement to have the spotlight, not the cues. Continue reading “Coaching & Cueing (Part 7 – Phases & Summary)”
Posted in Professionals |
By dr on November 16, 2015
Clinical
- “Knowing how to think empowers you far beyond those who know only what to think.” -Neil deGrasse Tyson
1) Great stuff from David Butler. He goes over tennis elbow and shares several manual and exercise treatments. A very generous post.
2) “Overextension refers to not just a position of one or more joints, but also a state of mind.” -Michael Mullin
3) Great post by Sian on patella tendinopathy. This article seems to cover all the current concepts with a clinical perspective. Continue reading “November Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on October 17, 2015
Clinical
- “Each time we introduce an assumption, we also introduce a new bias into the final solution” -Serge Gracovetsky
1) “Our neurological wiring has evolved into networks of patterned behavior designed to efficiently complete tasks mandated by the environment. Anatomy provides the frame to carry out these behaviors; the changes to structure are the tangible result of our habits. But once we open up some behavioral options for new habit formation, anatomical abnormalities don’t seem quite so concrete and problematic.”-Seth Oberst
2) Here’s the last category of the Coaching & Cueing series – Proprioceptive Cues
3) Want another tool for decreasing muscle tone? Try shortening the muscle and use some reciprocal inhibition.
The Gait Guys want you to decrease hypertonic muscles by stretching the antagonist? Interesting article on reciprocal inhibition and muscle spindles.
Erson wants you to try shortening the muscle for 30-60 seconds before you go aggressive. Continue reading “October Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on October 6, 2015
This is a very common intervention in movement coaching (whether the practitioner knows it or not). Simply changing an exercise to achieve the same goal is essentially a proprioceptive cue. Changing from a clamshell to a fire-hydrant can be a proprioceptive cue by altering the ascending sensory information during an isolated transverse plane glute strengthening exercise. Continue reading “Coaching & Cueing (Part 6 – Proprioceptive Cues)”
Posted in Professionals |
By dr on September 15, 2015
Clinical
1) Dan Pope shares another awesome video exercise progression – this time it’s on jump variations. He literally shows you how to bridge the gap in this one. Great stuff.
2) Leon Chaitow goes over pulsed muscle energy technique. A much safer and more effective intervention than cranking on joints with aggressive stretching. Take note of his communication in the video – calm, slow, speaking – external cues – takes his time to get the patient to perform exactly what he wants. #Variables
3) Tom Goom writes some of the best running articles out there. Here’s a great post on the importance of load capacity, the envelope of function, kinetic chain load, and the non-tissue issues. This might be the most important concept in rehab. Continue reading “September Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on September 2, 2015
Since our species is vision dependent ( >50% of cortex dedicated to processing visual information), visual cues can be an easy way to invoke a sensory change that alters movement patterns. This includes not only the sensory input from our external environment, but also our unique ability to create an internal vision (motor imagery). Continue reading “Coaching & Cueing (Part 5 – Visual Cues)”
Posted in Professionals | Tagged assessment, Prevention / Recovery |
By dr on August 15, 2015
Clinical
1) Read this one – the most detailed and thorough blog post on movement variability. Great stuff from Dave Tilley.
“With movement practice, it is believed by some that coordinative variability decreases (better able to synergies motor patterns for general movement planning) while elemental variability increases (more strategies to generate real time adjustments or handle different conditions while still successfully completing the given task or skill).” Continue reading “August Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on August 14, 2015
Our brain is quite complicated. It is constantly going through extremely complex processing to achieve many different outputs (movement, speech, vision, thoughts, emotion, pain, allostasis, etc.).
STRESS is one of the most influential factors on our brain’s ability to process efficiently. And in today’s society everyone has had it, many people live in it, and some people can never escape it.
Stress an epidemic and it will Continue reading “Problem & Solution”
Posted in Patients, Professionals | Tagged assessment, Nervous System |
By dr on August 2, 2015
Unfortunately, the rise in popularity of external cueing has led to a bad stigma of internal cueing. After reading the last article in this series you may be thinking why would you ever internally cue someone?
Here’s why: Continue reading “Coaching & Cueing (Part 4 – Internal Verbal Cues)”
Posted in Professionals | Tagged assessment |
By dr on July 15, 2015
Clinical
1) These are awesome – Dan Pope shares a very useful 2 part shoulder rehab progression with a ton of exercise examples (Part 1 – Closed Chain & Part 2 – Open Chain). And here’s his nice review of scapular dyskinesis.
2) Do you know when to use an External Cue? Do you know why? If not, here’s the answers – External Verbal Cues.
3) The Gait Guys teach you about Forefoot Supinatus – “A forefoot varus differs from forefoot supinatus in that a forefoot varus is a congenital osseous where a forefoot supinatus is acquired and develops because of subtalar joint pronation.” Continue reading “July Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on July 1, 2015
The type of cue one chooses should be based on the environment, individual, and task.
This article should help you understand when to best choose an external cue.
External Cue: focuses on how the body’s output affects the environment (outcomes, objects, etc.) Continue reading “Coaching & Cueing (Part 3 – External Verbal Cues)”
Posted in Professionals |
By dr on June 15, 2015
Clinical
1) Sure, it’s a dynamic system and the nervous system has a huge influence. But you can’t dissociate the physicality of our world from the human body. Simple biomechanics can have a profound effect on your patient’s movement. Here’s an example of how the first class lever works to Increase Glute Med Activity.
2) Don’t forget about the frontal plane aspect of the bunion deformity – “the degree of first metatarsal pronation is linearly related to the amount of medial deviation of the first metatarsal”
3) Kathy Dooley goes over the Obturator Externus – “When this muscle is locked long, it will contribute to hip compression. Since the muscle travels from the anterior outer pelvis posteriorly to the greater trochanter’s inner fossa, it works as a sling with obturator internus to keep that femur jammed into the acetabulum. “ Continue reading “June Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on June 15, 2015
We need to first clarify an important concept before we go into coaching and cueing:
- NOT ALL MOVEMENT REQUIRES COACHING
To Coach or Not to Coach
If someone is performing a movement/exercise correctly, all you have to do is shut your mouth and smile.
If someone is performing a movement/exercise incorrectly, you should ask yourself two questions: Continue reading “Coaching & Cueing (Part 2 – The Categories)”
Posted in Professionals | Tagged assessment, Biomechanics, Hip |
By dr on June 1, 2015
My co-worker was on vacation recently and I was seeing one of his chronic pain patients (years of pain). She was doing very well and was becoming independent in a full exercise routine. I did a quick evaluation and noticed one thing that she could improve on from a movement perspective. I didn’t use any dangerous pathoanatomical language. I just simply pointed out that she could be stronger if she kept her rib cage down when she performed certain exercises. We went over this cue a bit more with some basic proprioceptive exercises before she started her exercise program. Continue reading “Coaching & Cueing (Part 1 – Intro)”
Posted in Professionals | Tagged assessment, Core |
By dr on April 15, 2015
Clinical
1) Lately, I’ve been interested in the connection between vision and the cervical spine. Here’s two interesting articles I found this month.
“The direction of eye movements was horizontal when the sternocleidomastoidmuscle on one side of the neck and the splenius on the other side were activated, and downward when both splenii muscles were vibrated.”
“During neck rotation SCM and MF EMG was less when the eyes were maintained with a constant intra-orbit position that was opposite to the direction of rotation compared to trials in which the eyes were maintained in the same direction as the head movement.”
I put people in challenging developmental positions and have them use their vision to either increase motion or to dissociate their vision from their cervical spine (changing muscle activation patterns).
2) Still don’t think vision and the cervical spine are related? Check out this research article on Continue reading “April Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on March 15, 2015
Clinical
1) There’s a weird campaign by some Hipster PTs who are arguing that posture isn’t important. Maybe they’re doing it for social media popularity. Maybe what they’re really trying to say is that we shouldn’t create thought viruses. Maybe what they’re saying is that we shouldn’t blame all of our patients’ problems on a static postural assessment. Maybe they don’t understand that posture is a biobehavioral pattern. Regardless of their underlying point, dogmatically saying posture doesn’t matter is like saying physics and physiology doesn’t matter.
2) “From a sensory perspective, moving fast has a lot of sensory noise – it’s loud…By lowering the magnitude of the sensory stimuli, we can better perceive excessive muscular rigidity and help to regulate it.” – Seth Oberst
3) “The 90-90 hip lift says that the pelvis is too far forward, especially on the left and we would like to put it back to a neutral position and we are going to use a couple muscles to keep it there” –The Nominalist
4) Here’s a list of some DNS based exercises. Continue reading “March Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on March 1, 2015
I ran a secret experiment on our acupuncturist, Mila Mintsis.
But before I go into the details, Continue reading “My Secret Acupuncture Experiment”
Posted in Patients, Professionals |
By dr on February 15, 2015
Clinical
1) I first learned about the relationship between the pelvis and hip ROM from Chris Johnson – you can instantly increase hip IR on the table by having the patient posterior pelvic tilt. Then upon studying the concepts of SFMA, DNS, and PRI, I began to understand how the pelvis (as well as diaphragm/thorax/spine) influences the hips. Now I understand that most hip impingement patients are really pelvis patients, not femur patients. Mike Reinold wrote a concise and simple post on this concept here.
2) The Gait Guys go over the Continue reading “February Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on February 1, 2015
I was lucky enough to be invited to another one of Dan Park’s quality continuing education classes at Perfect Stride. This time it was for Functional Range Release (Upper Extremity) with Andreo Spina. I had been reading a lot about Spina’s work and was excited at the chance to learn about the FR/FRC techniques and principles. Continue reading “Andreo Spina’s Functional Range Release”
Posted in Professionals | Tagged assessment, Biomechanics, Prevention / Recovery, Review |
By dr on January 15, 2015
– January Hits –
1) If you are a manual therapist, please understand the current concepts of manual therapy. One of these concepts is that we cannot cause an immediate and permanent plastic deformation of tissues. So painfully digging into tissues to “release” them is really just another form of torture. Here are 3 Pain Free Manual Techniques from Erson – Pec Minor, Psoas, QL.
2) “Based on animal studies, it has been proposed that central sensitization associated to nociception (maladaptive plasticity) and plasticity related to the sensorimotor learning (adaptive plasticity) share similar neural mechanisms and compete with each other.”
3) Seth Oberst has a great read on hyperinflation and what to do about it (Part 1, Part 2). Continue reading “January Hits (2015)”
Posted in Professionals | Tagged The Hits |
By dr on January 1, 2015
One of the best things about the information age is the amount of great content out there. There are so many smart, generous individuals sharing information that can improve your skills and increase your quality of care. These blogs are accessible, straight forward, and clinically applicable. Here is my year end summary of some of my favorite stuff from this past year.
I came out of the stone-age and started using Google Analytics, which allowed me to see which of my articles were most popular, and which ones were only read by my girlfriend. It wasn’t what I expected.
Keep in mind that these lists are in no particular order. And also, this is just a small amount of the great articles out there. It’s just the ones I enjoyed the most from a years worth of Hits. If your favorites weren’t listed here, please feel free to leave a comment with your Top Reads. Continue reading “The Best of 2014”
Posted in Professionals | Tagged The Hits |
By dr on December 15, 2014
– December Hits –
1) Two great articles on placebos. The evolutionary history of placebos from Nicholas Humphrey – “when people are cured by placebo medicine, they are in reality curing themselves” – “The placebo effect is a particular kind of priming effect.” And how placebo helps pain from Todd Hargrove – “In other words, the placebo effect does not involve anything magical. It is one of many ways that our cognition affect our physiology.” – “The research of Benedetti and others has identified three different patterns of mental processes that create the placebo effect: (1) expectations of benefit; (2) reduction of anxiety; and (3) learning through association.” Continue reading “December Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on November 15, 2014
– November Hits –
1) Stress is stress. And there are many outputs that can occur in response to stress. Too often we get stuck obsessing over just one of the outputs – PAIN. As movement professionals we should focus on the output that we’re the most proficient at – MOVEMENT. If you disagree, Zac Cupples will convince you in this phenomenal article. “Assessing movement may be the simplest way to assess an individual’s stress status.”
2) Decreased hamstring strength increases ACL loading during sidestep cutting.
3) “If your tongue is on the roof of your mouth, you are connecting palate, pharynx, hyoid, jaw, and skull. You are stabilizing your airway, so you can breathe, while anchoring your TMJ so it doesn’t deviate. Now, your body is more balanced and can better ambulate.” –Kathy Dooley Continue reading “November Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on November 1, 2014
As many physical therapists have probably noticed, there is an increase in the amount of Crossfit athletes showing up in our clinics. This isn’t because it injures everyone. It’s because it’s becoming very popular and people love it.
We see the same thing happen during ski season and marathon season. It’s not necessarily the activity, it’s the increase in participation.
However, that’s not to say that it’s only an increase in participation that leads to a higher incidence of injuries. There are many other variables involved. Some of which can be improved upon to decrease the risk of injury.
I’ve noticed a few trends in my experience with Crossfit athletes. The crossfitters that tend to get hurt are the ones that seem to make the same 2 Mistakes: Continue reading “An Open Letter to Crossfit: The 2 Mistakes (Part I)”
Posted in Patients, Professionals | Tagged assessment, Biomechanics, Lumbar, Prevention / Recovery |
By dr on October 15, 2014
– October Hits –
1)A good soap box by Roger Kerry – “Calls to abandon a biomedical model is evidence-based moronicy. And downright dangerous.” – “Movement is everything.” – “Movement helps people contribute to society and it keeps the world going.” – “If you are a research funder, PLEASE STOP FUNDING RIDICULOUS RCTs.”
2) The Gait Guys take you down a static assessment rabbit hole with the functional anatomy of the lumbricals, flexor digitorum longus, and quadratus plantae. One of my favorite reads of the month.
3) Go Barefoot – “those feet should be straight-up sensory vacuums taking up as much sensory information as possible” -Seth Oberst
4) Adding single joint exercises to a multi-joint exercise program had no effect muscle thickness or peak torque production. #MovementNotMuscles Continue reading “October Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on September 15, 2014
– September Hits –
1) “Maintaining the short foot position can generate an arch and produce a monstrous feed-forward loop that maintains tension and stability throughout the system reinforcing to the brain that force can be safely produced. When the arch collapses the nervous system quickly downregulates in an attempt to avoid excess force thru the entire lower quarter while in an unstable position, yielding decreased output.” -Seth Oberst on foot positioning
2) Tendinopathy research goes pretty deep. There has been a lot of progress over the years, but there is still a ton we don’t know. Here are 2 posts to update your knowledge: 1) Peter Malliaras’s tendinopathy research post 2) 10 Clinical Pearls from ISTS 2014
3) Adriaan Louw and the ISPI just published a great study on pain education and how it can save the healthcare system a ton of money. Here is a quick flow sheet to understand the process. He also has a nice post on the important question, is it a tissue problem or a pain problem? Adriaan’s Medbridge course is worth the subscription alone. Continue reading “September Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on September 1, 2014
On August 2 and 3rd I was lucky enough to part take in Mark Cheng’s Prehab-Rehab 101 workshop at Perfect Stride in NYC. This was not only a special event because of the instructor and content, but it was the smallest class size I’ve ever been in. There were only 13 other clinicians in the class. Having this much of Mark’s attention provided for a great learning experience. Continue reading “Mark Cheng Prehab-Rehab 101 Workshop Review”
Posted in Professionals | Tagged Review |
By dr on August 15, 2014
– August Hits –
1) Does your patient suffer from VOMIT? It is one of the fastest growing pathologies in our society. Make sure you are aware of this terrible problem and educate your patients.
2) I’m not going to stop drinking it, but here’s some good information.
3) “Our study demonstrated no benefit for intramuscular PRP injections, as compared with placebo injections, in patients with acute hamstring injuries” Continue reading “August Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on August 1, 2014
Part I went over the benefits and disadvantages of the deep squat. In Part II, I will describe how I approach the squat in different settings and how I train it. Contrary to Part I, which was a collection of the current research and physiological facts about the squat, Part II is mostly empirical evidence and professional opinion. Continue reading “The Deep Squat (Part 2 – In the Clinic, In the Gym, How to Train it)”
Posted in Professionals | Tagged Hip, Knee, Lumbar, Pelvis / Sacroiliac |
By dr on July 15, 2014
– July Hits –
1) Have you heard about using isometrics to decrease pain associated with tendinopathies? I was unfamiliar with this concept so I thought I’d send out a tweet to one of the leading experts, Jill Cook. She gave some great advice that you can immediately use in your practice. Jill’s guidelines: Continue reading “July Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on July 1, 2014
Two of my favorite things to do in my practice are to assess movement patterns and use kettlebells. So when I heard about the amalgamation of FMS and StrongFirst I was pretty stoked. Throw on top that Gray Cook and Brett Jones were teaching the course, and it was my most anticipated course of all time. Continue reading “Foundational Strength Course Review”
Posted in Professionals | Tagged assessment, Prevention / Recovery, Review |
By dr on June 15, 2014
– June Hits –
1) “When an imparted load exceeds the load bearing capacity of the tissue accepting it, damage occurs. Neurological errors in movement execution commonly lead to loads being placed on “unprepared” tissues. It is therefore important to focus on two aspects of training to reduce the likelihood of sustaining injuries: 1. Working on improving neural control via progressively complex movement tasks – 2.Improve the physical, mechanical load bearing capacity of tissues.” – Andreo Spina
2) Some good PRI exercises in this article by CPG.
3) A story about a man amputating his own arm to try to get rid of his pain. It didn’t work. #PainScience Continue reading “June Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on June 1, 2014
The deep squat (aka full squat, aka ass to grass/ATG squat) is one of the most debated, talked about exercises/assessment we have in human movement. Some talk about the deep squat as if it’s the cure to cancer, some talk about it like it’s going to cause the apocalypse. I have found that Continue reading “The Deep Squat (Part 1 – The Good, The Bad, & The Not So Ugly)”
Posted in Professionals | Tagged assessment, Biomechanics, Knee, Review |
By dr on May 15, 2014
– May Hits –
1) Do you know about the anti-icing movement? Many are advocating against cryotherapy post injury. Some blindly jump on the bandwagon, some feel threatened and become defensive, and most of us just want to know why. I’ve recently come across a couple great articles on the theory and evidence that explains why we should not ice injuries. Even if you continue to ice, you should at least know what it really does (e.g. numbing effect, descending modulation, body temp regulation, placebo). Continue reading “May Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on May 1, 2014
I am a big fan of the FMS (Functional Movement Screen) and SFMA (Selective Functional Movement Assessment). Together these screens and their associated principles make up the Functional Movement Systems.
I’ve been using this system for a couple years and have had a lot of success with it. The more efficient I become at this approach, the more my outcomes improve.
I still have much to learn and am by no means an expert, but I thought I’d share the 4 biggest mistakes I see people make with the Functional Movement Systems. Continue reading “4 Mistakes People Make with the Functional Movement Systems (FMS/SFMA)”
Posted in Professionals | Tagged assessment, Biomechanics |
By dr on April 15, 2014
– April Hits –
1) This is a MUST READ for anyone that puts their hands on their patients. Erson shares 5 profound articles that changed his career.
2) StrongFirst Tactical Strength Challenge Program
3) “Think of PNF as a way of means of feeding the sensorimotor system specific purposeful information to create a purposeful and functional motor strategy” – Ramez Antoun
4) Post-Activation Potentiation – A phenomena by which Continue reading “April Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on April 1, 2014
Part I went over stress, tissues, the nervous system, and many of the factors that are involved with recovery.
Throughout a PT session there are many opportunities to influence the patient’s health; both for the immediate and long term effects. This post will go over the 4 factors of recovery that I often try to discuss with patients before they are discharged from Physical Therapy. Continue reading “The Art of Recovery (Part 2 of 2)”
Posted in Patients, Professionals | Tagged Prevention / Recovery |
By dr on March 15, 2014
– March –
1) Communication is just as important as the intervention. Seth Oberst writes a great post on the difference between external and internal cues. “It’s now being shown that athletes focusing on the results of the movement are producing more force, jumping higher, generating better performance in stressful situations, and increasing fluidity and multi-tasking.”
2) Evolution has shown us the importance of diet and the jaw on our growth as a species. Here’s an interesting site on the jaw and it’s relation to the co-morbidities.
3) Want to learn how to pistol squat? Click here. Continue reading “March Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on March 1, 2014
One of the most difficult questions to answer in rehab is: “when will I get better?”
Coming out of grad school my response was usually mumbling some ridiculous time period with a deer in the headlights look on my face. I had no idea. I knew the tissue healing timetable…and that was about it. I had little experience with specific injuries and didn’t yet understand the complex, multi-faceted factors that influence recovery.
Now I’m a little better at hiding that deer in the headlights look, I have more clinical experience, and I know more about the art of recovery. Continue reading “The Art of Recovery (Part 1 of 2)”
Posted in Professionals | Tagged assessment, Prevention / Recovery |
By dr on February 15, 2014
– February –
1) One of the best things about PRI is their interdisciplinary approach. They’ve done a great job at providing holistic care. Specifically, PRI Vision is putting out some great stuff. PT’s have been stuck advising the same ergonomics with the same reasoning for the past 30 years. Heidi Wise goes over a more methodical way to address your patient’s ergonomics (Part 1 & Part 2).
2) Kevin Carr goes over some great Row Progressions. Use these for your patient. Use these for yourself in the gym.
3) The language you use with your patient has a huge impact. Be positive and optimistic. Don’t talk over their heads. Don’t scare them with patho-anatomy and diagnoses. Continue reading “February Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on February 4, 2014
In the past 10-20 years there has been a trend towards stabilizing the proximal joint. Everything seems to be going more and more proximally. And this is a good thing! It is providing us with better outcomes and quicker pain free rehabilitation.
If you look at the knee joint you can see the progress. We’ve gone from isolated patella mobs and VMO strengthening to hip strengthening. And now we are going even further up the chain and looking at lumbo-pelvic complex.
The same thing is happening with the shoulder. We’ve gone from isolated thera band ER/IR to scapula stabiliztion. And now we are going even further and looking at the thoracic spine and ribs.
And if we go just 1 step further at both joints we end up where it all began in the first place…the core. Continue reading “Everything is Moving Proximally”
Posted in Professionals | Tagged assessment, Core, Hip, Lumbar, Pelvis / Sacroiliac, Prevention / Recovery, Shoulder |
By dr on January 19, 2014
– January 2014 –
1) Pain and Central Sensitization is a growing topic in our field. And for a good reason, pain is the #1 reason people come to see us. Plus, chronic pain is becoming more and more common. It’s great having so much information available to learn about these topics, however, there isn’t a lot of information on the specific clinical application. I sought out pain expert, Adriaan Louw, to answer some clinical questions on pain science in this months post.
2) Charlie Weingroff goes over some theory on why ankle mobility is important for glute activation. He also has a great article on how different body types tend to move and perform. Continue reading “January Hits (2014)”
Posted in Professionals | Tagged The Hits |
By dr on January 1, 2014

Adriaan Louw, PT, PhD, CSMT
Adriaan Louw is a busy man. Between running ISPI (International Spine & Pain Institute), performing research, treating patients, drinking beer, and watching football he doesn’t have a lot of free time. However, he was kind enough to answer some quick questions to help me understand pain, central sensitization, and the clinical application of neuroscience. As always, his answers were very helpful and I thought I’d share them with everyone else. Continue reading “11 Questions with Adriaan Louw”
Posted in Professionals |
By dr on December 15, 2013
The Hits
1) Human movement isn’t always as simple as basic kinesiology and anatomy. James Speck gives a great example of this in his detailed article describing the soleus as a knee extender. “When a muscle contracts, it doesn’t think about which direction in needs to pull. It just shortens.”
2) More on pain science: “…they used newer MRI technology to see how flexible people could be in responding to pain. The mind-wanderers were more flexible.” Pain isn’t a pathological structure; it’s a central processed perception.
3) I recently had a medial elbow tendinosis patient. When I screened him with the SFMA his single leg balance was terrible. He had some severe ankle/foot stability deficits. This study was in a recent JOSPT. Regional interdependence. SFMA. Continue reading “December Hits (2013)”
Posted in Professionals | Tagged The Hits |
By dr on December 1, 2013
I have been following Erson Religioso, a PT and blogger, for quite some time now. He has repeatedly (no pun intended) discussed the effectiveness of Mechanical Diagnosis & Therapy (The McKenzie Method or MDT). He’s a very knowledgable clinician and runs his social media with integrity. Over the years he has provided a great deal of clinically applicable information and I have seen results in my practice using some of his methods.
I decided I had to check out MDT first hand and learn about their method. This past July I took McKenzie Part A – The Lumbar Spine with Dave Oliver. Continue reading “23 Things I Learned From McKenzie Part A”
Posted in Professionals | Tagged assessment, Lumbar, Pelvis / Sacroiliac, Review |
By dr on November 15, 2013
-OverheadShoulder-Jerk-ALL-Hammy-Memory-FrontSquat-Speed-Mistakes-GMI-LowerTraps-Pain
1) Down and back isn’t always right for our shoulder patients. In fact, some people need the opposite. This months article goes over how to assess and treat someone for overhead shoulder exercises.
2) This is awesome – slow-mo clean & jerk video with analysis from olympic lifting coach Jim Schmitz.
3) A new knee ligament? Researchers have found an Anterolateral Ligament (ALL) in the knee. Is this a profound advancement in anatomy? Or is this just a carved out fascial thickening?
4) Great perspective on hamstring tightness. Mike Reinold discusses how a tight hip flexor can pull the pelvis into an anterior pelvic tilt, thus decreasing the contralateral straight leg raise. You could use the 90-90 active posterior chain test in hooklying to further Continue reading “November Hits”
Posted in Professionals | Tagged The Hits |
By dr on November 1, 2013
In Part I you learned the concepts behind upward rotation and the overhead shoulder. This article builds off of these concepts and will show you how to properly assess and treat for the overhead shoulder.
I cannot emphasize enough how important a thorough assessment is before prescribing overhead shoulder exercises. Without an assessment to determine any impairments or movement dysfunctions you will not be able to properly prescribe the correct exercises. Before someone starts overhead movements you should make sure they’re clear in all of the overhead shoulder characteristics (Part I). Failure to do so could result in injury. Continue reading “The New Overhead Concept (Part II)”
Posted in Professionals | Tagged assessment, Shoulder |
By dr on October 15, 2013
– Upper Trap – Thought Viruses – Deadlift – 5×5 – Reciprocity – Sensory Fascia – E5 – Perception – Anti-Valgus – Bad Medine – Cook’s 3’s – Doga
1) The poor upper trapezius. It might be the most understood muscle in the body. It’s not a major shoulder elevator and it isn’t a big problem in shoulder patients. In fact it’s usually the opposite. Check out this months post to learn more. Continue reading “October Hits”
Posted in Professionals | Tagged The Hits |
By dr on October 1, 2013
Traditional Down & Back
At this point we all know the importance of a stable and strong scapula for shoulder function. Almost every PT, athletic trainer, and personal trainer trains the shoulder with a “down and back” cue. This cue allows for a better stable position of the scapula and enables the rotator cuff to work more effectively. Kolar has summed this concept up in a single sentence: Continue reading “The New Overhead Shoulder Concept (Part I)”
Posted in Professionals | Tagged Biomechanics, Prevention / Recovery, Shoulder |
By dr on September 16, 2013
Kettlebells – Runners – Habits – Longevity – Med Ball – Tightness – Goblet – Yoga – Elbow Grease
1) Kettlebells are becoming more and more common in fitness and rehab. If you don’t use them, you should. Here’s this months article on my expirience at the premier kettlebell workshop.
2) Erson goes over 5 things to look for in runners. “Running is one sport that arguable needs more symmetry than most. I tell my runners it’s because you’re doing the same thing over and over for 1000s of steps until you stop!” Continue reading “September Hits”
Posted in Professionals | Tagged The Hits |
By dr on September 1, 2013
On June 1st I had the pleasure of participating in a StrongFirst Kettlebell Workshop with Phil Scarito. It was a 1-day course that went over the intricacies of the basic kettlebell movements (Deadlift, Swing, TGU, Goblet Squat, Press). The theory is that it’s better to master the fundementals than to be average at a bunch of different lifts. Plus, it’s these basic KB movements that that have the greatest impact on improving one’s physical abilities and movement patterns. Continue reading “Course Review – StrongFirst Kettlebell Workshop”
Posted in Patients, Professionals | Tagged Hip, Knee, Prevention / Recovery, Review |
By dr on August 15, 2013
– Lumbar Extension – Selling – Pain&Expection – Evolved Shoulder – Posterior Hip Pain – Posterior Chain – Gray Cook – EBP? –
1) Our profession and our society has become so afraid of lumbar flexion that it’s almost a phobia. This obsession of avoiding lumbar flexion has allowed another problem to slip by – excessive lumbar extension. I’ve been noticing more lumbar extension dysfunction in the clinic. Read about it in this months post here.
2) The more I practice the more I start to think the most important aspect of PT is the patient’s mindset. I look for 2 things in the eval Continue reading “August Hits”
Posted in Professionals | Tagged The Hits |
By dr on August 1, 2013
Low back pain is one of the most common injuries we see. Traditionally you always hear a lot of information regarding excessive lumbar flexion. And with the amount of information readily available in our society, many patients already know this as well. This has caused some therapists and patients to walk around terrified that the next time they bend over their L5-S1 disc will splatter against the wall behind them. But what about the other direction? What about the potential problems in extension patterns?
We’ve concerned ourselves so much about “blowing out a disc” with flexion that we’ve completely overlooked extension problems. Continue reading “Lumbar Extension Dysfunction”
Posted in Professionals | Tagged assessment, Hip, Lumbar, Pelvis / Sacroiliac, Prevention / Recovery |
By dr on July 16, 2013
– Fatigue – High Heels – Motor Learning – Mobility – Threshold – Strengthening – Parachute – Protocols – Armbar – Neuro –
1) I think exercise programs like crossfit and P-90X are great. They get more people moving and interested in their health. And in today’s society, decreasing the amount of sedentary people is very important. However, when exercises are performed past failure a ton of things go wrong. A new study showed there is a deterioration of lower extremity biomechanics when fatigue hits. This causes a dangerous cascade of events: compensations, inefficient movement, substitution movement patterns, and an increased risk for injury. While many of us already know this, many of our patients don’t. Educate them. Continue reading “July Hits”
Posted in Professionals | Tagged The Hits |
By dr on July 1, 2013
Understanding the difference between low and high threshold strategy is a very important part of rehab and training. If a patient is using the wrong strategy for the task they will not only be inefficient, but they can make the injury worse and cause more harm. Continue reading “Low vs. High Threshold Strategy”
Posted in Professionals | Tagged assessment, Prevention / Recovery |
By dr on June 17, 2013
– Butler Cliffnotes – Deep Squat – MDT Reset – Hip Thrust – Hamstring Strains – DNS & Powerlifting –
1) So Zac Cupples does Cliffnotes for PT books. Here’s his post on the Sensitive Nervous System by David Butler. If you aren’t familiar with Butler and the NOI approach you should check it out. “Pain is an unpleasant, sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage.”
2) As a deep squat advocate, I loved this post by James Speck. To perform the deep squat you must have BOTH mobility and stability. This alone makes it a great assessment and intervention. Continue reading “June Hits”
Posted in Professionals | Tagged The Hits |
By dr on June 1, 2013
The quadruped position is a very important developmental posture. From this posture we learn to crawl and transition to half-kneeling (which then transitions into standing). Through this posture we develop core, shoulder, and hip stability, learn reciprocal UE/LE motion, and begin to control our spine through our weight-bearing extremities. The quadruped position has many details that are often lost or forgotten when training. Mastering these subtleties and progressing within the edge of your ability will lead to a great effect on your stability. Continue reading “Quadruped”
Posted in Professionals | Tagged assessment, Cervical / Neck, Core, Hip, Lumbar, Pelvis / Sacroiliac, Prevention / Recovery, Shoulder |
By dr on May 16, 2013
Language – Hip Hinge – Ankle/Hip – Weingroff – Boyle – Core Exercise – Knee Valgus
1) “An alteration of the language output may be as clinically potent in desensitising pain neurosignatures and it certainly has not been considered as deeply in rehabilitation.” David Butler discusses how correcting patients language & thoughts relating to their pain is just as important as it is to correct their movement output. This month’s JOSPT has a related article on the how movement system diagnostic labels can prevent the disconnect between diagnostics and treatment processes that pathoanatomic labels create.
2) The hip hinge is one of the most important movement patterns for anyone that moves. This months article goes over what it is, how to assess it, and how to correct it. Continue reading “May Hits”
Posted in Professionals | Tagged The Hits |
By dr on May 3, 2013
The hip hinge is a basic movement pattern that everyone must have. When people have atrophy of this movement pattern they end up compensating in all sorts of ways (trendenlenberg, dynamic valgus, knee dominant movements, lumbar flexion). This leads to decreased performance and increased risk for injury. Continue reading “Hip Hinge”
Posted in Professionals | Tagged assessment, Hip, Lumbar, Pelvis / Sacroiliac |
By dr on April 15, 2013
Joint Laxity – Davis’ Law – Deep Squat – Foot Types – Standing Help – Step Up
1) Beighton Laxity Scale gives a good indication of your patients congenital laxity. If your patient is extremely hypermobile then you shouldn’t be spending alot of time doing joint mobilizations and/or manipulations. These patients require a great deal of stability.
2) Davis’ Law, the soft tissue equivalent to Wolff’s Law, describes how soft-tissues adapt to stress. It describes how muscles adapt in a reciprocal manner. For example, a strong and inflexible gastroc will usually cause the anterior tibialis to become weak and flexible. With this law in mind, you should always consider the antagonist when trying to achieve an increase in strength or mobility. Continue reading “April Hits”
Posted in Professionals | Tagged The Hits |
By dr on March 15, 2013
5 Ways to Expand – Lateral Stability – Video Analysis – RTC Myths – Breathing – SIJ – Carbs
1) PT School lays down the necessary foundation to develop your career. There are many important things that we don’t learn in school. Erson goes over 5 of these things. I completely agree.
2) This might be a nice progression for patients that have already mastered the sagittal plane and have topped out with isolated hip strengthening (bridges, clamshells, side-step, etc.). Eric Cressey goes over advanced lateral stability training.
3) Chris Johnson goes over the details of how to videotape your runners for analysis.
4) Mike Reinold describes his 4 RTC myths in this article. Mike makes a great point on Continue reading “March Hits”
Posted in Professionals | Tagged The Hits |
By dr on March 4, 2013
Part I of this series dealt with breathing anatomy and mechanics. Knowledge and understanding of the anatomy and mechanics of breathing is essential for a proper assessment and intervention. This post will expand on the previous post and go over some indications, assessment, and intervention for breathing. Continue reading “Breathing – Part II – Indications, Assessment, & Intervention”
Posted in Professionals | Tagged Core, Lumbar, Pelvis / Sacroiliac |
By dr on February 15, 2013
Breathing – Thoracic Mobility – FMS – Neuro – Pendulum Theory – Warm-Up – Glutes
1) Bill Hartmen uses the downward dog to increase pre-load on the diaphragm, activate the serratus anterior, and unload the scalenes while facilitating deep neck flexors. All this can significantly help your breathing patterns. Check out this months post on breathing.
2) This is a great thoracic mobility technique using the NMT T-Bar. A good way to increase thoracic mobilization and
integrate with scapular movement.
3) Nice summary of FMS corrections (from Mike Reinold’s site). Continue reading “February Hits”
Posted in Professionals | Tagged The Hits |
By dr on February 1, 2013
The average person takes about 21,000 breaths a day. This makes it one of the 3 biggest aspects of our patients life that we can have a profound effect on (other 2: posture & walking).
This post will discuss the holistic effects of breathing, anatomy, and the important cascade of events for proper breathing and inner core stabilization. Continue reading “Breathing – Part I – Anatomy & Mechanics”
Posted in Professionals | Tagged Biomechanics, Core, Hip, Lumbar, Pelvis / Sacroiliac, Prevention / Recovery, Shoulder |
By dr on January 15, 2013
Coordination – TRX Y’s – Nocebo – Hallux Mobility – Neuro Approach
1) Maybe we should slow down a little bit. Todd Hargrove goes over why slow movement is important for coordination and movement efficiency. This can be very useful when attempting to teach the “motor morons” how to move right. I specifically liked the Weber-Fechner Law, which describes that the relationship between the physical magnitiudes of a stimuli and the perceived intensity of the stimuli.
2) Overhead movements are usually butchered by patients. When trying to activate the lower trap many patients compensate with a rib cage flare, hyperlordosis, forward head, and unusual grunts. Cressey quickly goes over how to teach the TRX Y’s in this 2 minute video. Continue reading “January Hits”
Posted in Professionals | Tagged The Hits |
By dr on December 17, 2012
Pain – Deadlift – IPSI – Ankle Torque – Front Squat
1) Pain is usually the main reason why patients come to see us. The traditional orthopedic approach always uses a pathoanatomical explanation for pain, but this might not always be correct. Lorimer Moseley gives a very entertaining presentation on explaining pain. My recent post also goes over some of these central processing mechanisms. And Todd Hargrove has a great review (part 1, 2, 3, 4) of Moseley and Hodges conference on pain and this neurologic approach.
2) The dead lift is an essential movement pattern. It is hip hinging at it’s best. Gray Cook and Brett Jones go over the dead lift and some great variations with kettlebells. If you think the dead lift is a bad exercise than Continue reading “December Hits”
Posted in Professionals | Tagged The Hits |
By dr on December 3, 2012
On November 3rd & 4th I had the pleasure of taking the NeuroOrthopedic Institue course – Mobilisation of the Nervous System. I was lucky to have Adriaan Louw as the course instructor. I learned a tremendous amount over the weekend and returned to the clinic on Monday with an additional approach to treat patients with. The NOI provides a paradigm shift in the way we view the nervous system and pain. While it is impossible to cram a weekends worth of great information and techniques into a post, I’ll try to provide some key points I learned from the course. Continue reading “NOI – Mobilisation of the Nervous System”
Posted in Professionals | Tagged assessment, Review |
By dr on November 16, 2012
November Hits
Eccentrics – TPI – Foot Intrinsics – Rib Cage – Upward Rotation – Cubiod
1) My co-worker, Michelle Briancisco, has been talking about using eccentrics to increase ROM for years. She has found it really works well when patients aren’t responding to traditional muscle lengthening techniques. She hypothesizes that it neurologically alters the afferent motor output and also provides the patient with a sense of control during the lengthening.
2) Saw this on Erson’s site. I remember doing this at the TPI course. There’s a plethora of good shoulder warm up exercises to choose from for your patients. Continue reading “The Hits”
Posted in Professionals | Tagged The Hits |
By dr on November 7, 2012
I’ve been in over 25 clinics and worked with over 75 physical therapist. While this helped me gain knowledge and experience in the field, it has also shown me the different “types” of physical therapist out there. Most PT’s are great clinicians and want to help people to the best of their knowledge. However, there are some PT’s out there that become “that guy”. If you’ve worked in a couple different practices or if you think back to PT school you have probably met one of these “guys”. There are 3 types of “that guy” in the PT world: the hipster PT, the research snob PT, and the ancient PT. It’s fun to humorously classify these types of PTs, but it’s also important to make sure you don’t become one of them. Continue reading “Don’t Be “That Guy””
Posted in Professionals | Tagged Review |
By dr on October 15, 2012
October Hits
Atlas Glide – Turkish Get Up – Pelvodiaphraribcage – High Ankle Sprain – Deadlifts
1) The suboccipitals and occiput-atlas articulation are paramount when it comes to normal cervical function. The fact that our society is spending an increasing amount of time in the forward head posture makes this area even more important for cervical patients. Adding THIS to my soft-tissue work when appropriate has been very helpful.
2) Everyone seems to be talking about the Turkish Get-Up (TGU) these days. I’ve been adding more kettlebells into my own workouts and have been working on the TGU. It’s much harder than it looks when done correctly. It takes a great deal of mobility and stability throughout the entire body to complete it without compensations. Mike Roberton has a great step-by-step and Gray Cook has a video demonstration. Continue reading “The Hits”
Posted in Professionals | Tagged The Hits |
By dr on September 29, 2012
It is widely known that hip strenthening plays a significant role in the rehabilitation of knee pain. When it comes to our sagittal-plane loving runners the hips become even more of an issue. However, in 2011 Wiley and Davis published an article in JOSPT that found hip strengthening alone was not enough to alter running mechanics. This gave movement hipsters and research snobs more fuel to trash talk exercises that aren’t “functional” or that “research shows” it doesn’t elicit some desired EMG number. While I find remedial exercises to be an important step in rehab, I do agree that there needs to be a better transition between rehab and sport specific training. Continue reading “Functional Hip Strengthening”
Posted in Professionals | Tagged assessment, Hip, Prevention / Recovery |
By dr on September 15, 2012
September Hits
Popliteus – Hamstring Syndrome – Gray Cook – Calf Strain – Pavel Tsatsouline
1) The popliteus is an important structure of the knee that is often overlooked by many clinicians. While it may not be the main contributor to knee dysfunction, it can still have a major impact. Some patients need greater activation of this muscle, while others
benefit from a release. This is a good post on the popliteus and it’s functional role in the knee joint.
2) I recently had a patient with hamstring syndrome. She had been previously mis-diagnosed with piriformis syndrome, ischogluteal bursitis, lumbar radiculopathy, and hamstring tendonosis. Understanding how to differentially diagnose these patients may lead to a more specific treatment and a better outcome. Continue reading “The Hits”
Posted in Professionals | Tagged The Hits |
By dr on July 27, 2012
Regardless of the patho-anatomical etiology, most shoulder injuries involve a disruption in the delicate subacromial space (SAS). Once this space is altered the structures (joint capsule, articular cartilage, rotator cuff, biceps tendon, bursa) have increased risk for damage and misuse. This also leads to subsequent changes in muscle length-tension relationships, arthrokinematics, and motor patterns. Continue reading “Subacromial Space”
Posted in Professionals | Tagged Shoulder |
By dr on May 12, 2012
The half-kneeling position is a great way to assess and treat your patients hip and core stability. While it seems like an easy exercise, it has many subtleties that can make or break the position. Having a greater understanding of the half-kneeling position will help ensure that your patient achieves the maximal benefit. Continue reading “Why You Should Use the Half-Kneeling Position”
Posted in Professionals | Tagged assessment, Core, Hip, Lumbar, Pelvis / Sacroiliac |
By dr on April 8, 2012
This past month I had the pleasure of taking a University of St. Augustine continuing education course with instructor Larry Yack. The course went over spinal evaluation and manipulation (skilled passive movement of a joint). There was a tremendous amount of useful information and techniques. Here’s some random notes. Continue reading “Paris Course – S1 – Spinal Evaluation & Manipulation”
Posted in Professionals | Tagged Lumbar, Review |
By dr on February 15, 2012
When prescribing home exercises for my patients I often try to keep it to a minimum of 3 exercises. I understand it’s the last thing people want to do at the end of a long day, especially when they require great effort and concentration. Luckily for those of us that experience pain and discomfort there is an exercise that is easy to perform, doesn’t require a great deal of mental energy, and gravity does all the work for you. Continue reading “Constructive Rest / Passive Alignment / 90-90 Position”
Posted in Patients, Professionals | Tagged Lumbar, Prevention / Recovery |
By dr on December 28, 2011
Dynamic Stabilizers of the glenohumeral joint include the contractile tissues and the associated sensorimotor system involved with proprioception, kinesesia, and the sensation of resistance. For optimal shoulder stabilization the dynamic stabilizers must be working in an efficient synergistic fashion. Continue reading “Shoulder Stability – Dynamic Stabilizers (3 of 3)”
Posted in Professionals | Tagged Shoulder |
By dr on November 30, 2011
Force Closure
Force closure is a biomechanical myofascial system that helps to produce a “self-locking” mechanism for joints. It occurs when contraction of the muscles/fascia that cross a joint results in increased stability of the joint. This external dynamic myofascial force can increase stability by producing a closed pack articular position (increased congruency), generating segmental stiffness, and increasing compression perpendicular to the joint. Continue reading “Force Coupling for the Lumbo-Pelvic-Hip-Complex”
Posted in Professionals | Tagged Lumbar, Pelvis / Sacroiliac |
By dr on November 14, 2011
Static stabilizers are the non-contractile tissue of the glenohumeral joint. They are very important in shoulder stability at end-range ROM and/or when there is a dysfunction of the dynamic stabilizers. These static stabilizers set the base of support for the shoulder joint. Continue reading “Shoulder Stability – Static Stabilizers (2 of 3)”
Posted in Professionals | Tagged assessment, Shoulder |
By dr on October 16, 2011
It doesn’t take a subscription to a peer-reviewed medical journal to gain knowledge and understanding in the orthopedic world. Today there is a plethora of websites and blogs with so much free information that you can practically get free continuing education online. Here’s a list of some helpful sites. I’ve tried to focus on the ones that are more focused on concepts and education instead of product placement and marketing. Let me know if there is anything I’m missing.
Continue reading “Links”
Posted in Patients, Professionals | Tagged Links, Review |
By dr on October 4, 2011
The shoulder is one of the most complex joints in the human body. It has an amazing amount of inherit mobility, which in turn requires an adequate about of dynamic and static stability to function. Then if you consider the manner in which we use our shoulders and the lack of anatomical support, it’s easy to see why Continue reading “Shoulder Stability (1 of 3)”
Posted in Professionals | Tagged Shoulder |





{kind=link}
{kind=link}