Understanding the difference between low and high threshold strategy is a very important part of rehab and training. If a patient is using the wrong strategy for the task they will not only be inefficient, but they can make the injury worse and cause more harm.
Unfortunately, this has happened to all of our patients at one time or another. We give them a simple exercise like single leg balance, look away for a second, and turn back to see them holding their breath and violently flailing their arms to keep their balance. They’re not developing stability, they’re just using a dysfunctional high-threshold strategy to teach their body how to compensate with the wrong muscles.
If you understand the difference between the 2 strategies, you can prevent this from happening to your patients.
Quick Definitions:
Low-Threshold Strategy: Slow, tonic, local stabilizer, stabilizing muscle contractions that are for low-load tasks and reflexive postural control. This is necessary for joint centration.
High-Threshold Strategy: Fast, phasic, prime mover, global mobilizer, mobilizing muscle contractions that are for high-load tasks and force production. This is necessary for strength training.

Low-Threshold (Left), High-Threshold (Right);
Lebron wouldn’t be able to pull off the best block of the season if he didn’t have a strong fundemental low-threshold strategy to use an insane high-threshold strategy off of (note the lack of lumbar/T-L junction hyperextension).
5 Major Points
- The difference between high and low-threshold is one of the most important parts of the exercise continuum
- Low-Threshold must occur prior to High-Threshold to stabilize and centrate the body
- High-Threshold is necessary, but can become dysfunctional with poor training strategies
- Assess for threshold strategy by looking at breathing, posture, and alignment
- Build programs to encourage a fundamental low-threshold strategy before starting high-threshold exercises
Motor Units & Threshold Strategies
Motor Unit
High and low threshold strategy refers to the type of motor unit activity driving a task. These motor units are responsible for muscle contractions. The type of motor units recruited for a task are based on many different factors including: muscle fiber type, role of muscle, motor pattern, firing rate, and recruitment threshold.
Threshold Strategies
It’s important to understand that most local stabilizing muscles have a higher portion of low-threshold motor units, where as global moving muscles have a higher portion of high-threshold motor units. Further more, motor units are recruited sequentially from low to high. It’s the body’s way of being efficient and trying to perform a task with the easiest motor program possible. So before high-threshold motor units are recruited, all of the other motor units must be recruited (high-threshold on top of low-threshold). This increases the mechanical advantage of the global movers and centrates the joint, thus making it more efficient to perform the task.
- Low-Threshold Strategy MUST be recruited before High-Threshold Strategy.
Exercise and Thresholds
To put it in perspective you can look at single leg balance. You should be able to stand on one leg using a low-threshold strategy. However, if you add medicine ball throws or step-ups to a single leg stance you are going to have to use a high-threshold strategy on top of a low-threshold strategy. A low-threshold strategy alone is not strong enough to create enough force to throw a heavy medicine ball.
Low-Threshold & High-Threshold
Before you go crazy trying to label each movement and exercise, it’s important to note that this is a continuum. Not every movement is going to be exclusively one type of motor strategy.

Extremes of the Threshold Continuum Developmental Patterns = Low-Threshold Strategy Powerlifting = High-Threshold Strategy
Low-Threshold
Working within the edge of ability and gaining fundamental stability is paramount for developing efficient stability and power. Unfortunately many clinicians and trainers overlook this low-threshold motor strategy.
Here’s an example. I had an acute low back patient who was deadlifting 350 pounds. He could touch his toes, passed the ASLR test, his hips were strong, and he could hold a plank for hours. But when I took him through some low-threshold developmental stability patterns he started shaking all over the place. After he developed some low-threshold stability he went back to pain-free deadlifting and improved his PR by 20 pounds in the next month. It’s not always this extreme, but shows a great example of how joint centration goes beyond rehab.
So there are 2 ways you can sell this to your patients:
Optimist: If you are really strong without a low-threshold motor program, then imagine how much stronger you would be with one.
Pessimist: If your strong without a low-threshold motor program, then all you did was strengthen your compensations and poor movement patterns.
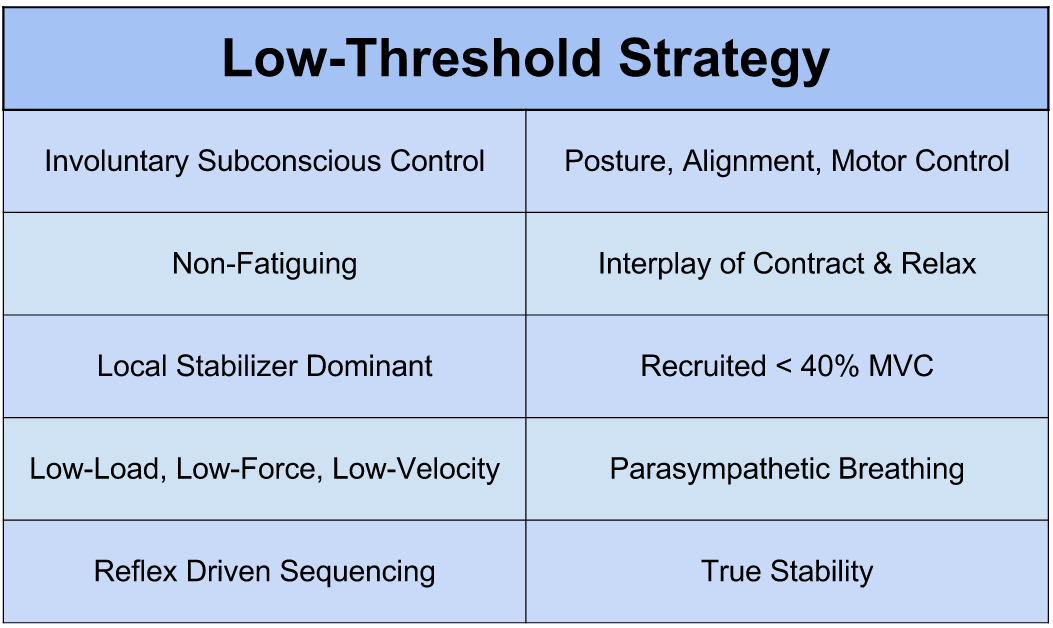
Characteristics of Low-Threshold Strategy
High-Threshold
Some people use the term high-threshold strategy to define a dysfunctional motor strategy. I feel that this can be a little misleading and give high-threshold motor patterns a bad rap. If athletes didn’t use high-threshold strategies they wouldn’t be able to accomplish the amazing physical feats we see on Sports Center’s Top 10. And without high-threshold strategies our Top 10 would just be a bunch of trick pool shots and geriatric shuffleboard.
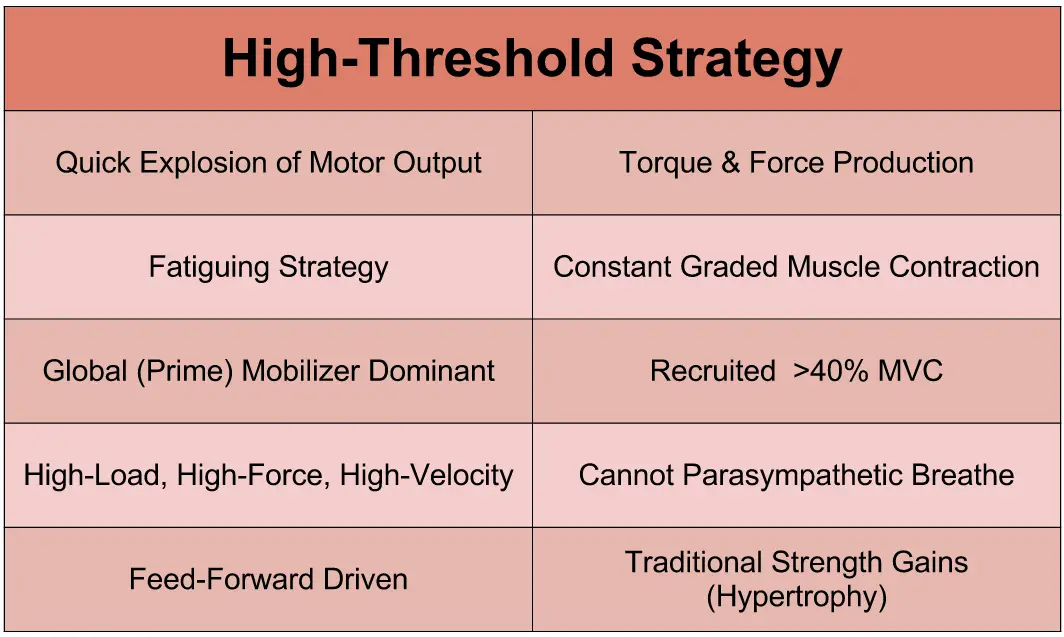
Characteristics of High-Threshold Strategy
What Goes Wrong?
The body moves very efficiently when the low-threshold precedes the high-threshold. It’s when people skip the low-threshold step that things start to go very wrong. This dysfunctional high-threshold only strategy will plague the body compensations and inefficient movement.
When the body fatigues and the local stabilizers stop firing, the body goes into a dysfunctional high-threshold strategy. This is filled with poor movement patterns. To make matters worse, it teaches the body how to incorrectly use global mobilizing muscles (as movers AND stabilizers). So now these muscles are always on and always trying to do everything, even for low-load activities.
Just like anyone that is worked twice as hard, these muscles get very unpleasant. They lock up, have overdeveloped tone, become fibrotic, have decreased blood supply (from being contracted all the time) and become over facilitated.
Cranking on these muscles may provide temporary relief. But to solve the problem you need to go to the low-threshold strategy that isn’t firing. Other wise the viscous cycle will continue.

Another kind of dysfunctional high-threshold strategy (note Homer’s loss of T-L junction stability and extended cervical spine, as well as Bart’s moro reflex).
High-Threshold Strategy is a Dysfunctional Pattern When:
- Used in Substitution of Low-Threshold
- Cannot Turn Muscles “Off” (Results in Splinting, Not Stabilizing)
- Global Mobilizing Muscles Have to Move AND Stabilize
- Places the Body in Poor Alignment / Posture
- Sacrifices Mobility for Force Production
So how do you assess for which strategy is being used?
The simple answer is breathing. 99% of the time breathing strategy it will match up with their threshold strategy.
The Threshold-Breathing-Continuum: Parasympathetic diaphragm breathing is used in low-threshold strategies. Breath holding and valsalva is used in high-threshold strategies.
- Assessing Breathing = Assessing Threshold Strategy
Another give away for dysfunctional threshold strategy is poor alignment/posture. If someone can’t use a low-threshold strategy they’ll compensate with a high-threshold strategy and the global mobilizing muscles will pull the body out of optimal positioning (centration).
So What Do You Do Now…?
FMS Performance Pyramid
The FMS Performance Pyramid provides a great picture of how to balance your plan of care (or training) in terms of human performance. Much like the low before high-threshold principle, this pyramid emphasizes the fundamental mobility balance, and coordination.
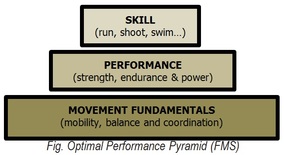
FMS Performance Pyramid
My Threshold Pyramid
It’s important to first consider mobility before threshold strategies. Mobility and tissue quality is a priority before stability and movement. Trying to force patients through mobility deficits will only feed into their movement pattern dysfunction. Once you have resolved or made a change in their mobility, you should then move towards threshold training.
Since the normal firing pattern is low-threshold before high-threshold, you should probably train your patients the same way. To do this, simply make sure your patient can perform low-threshold strategies independent of load, force, or movement. After this is accomplished you can add in the load, force, or movement and work towards more high-threshold type of strengthening exercises.
Once they are efficient with the low-threshold patterns don’t throw them away and forget about them. They’re great for warm-ups, CNS resets, starting positions, or active rest.
Examples of Low-Threshold → High-Threshold:
Core: Soft Rolling → Hard Rolling
Shoulder: Bottom-Up Kettlebell Screwdriver → Single Arm Rows
Hip: Quadruped Alt UE/LE → Deadlift
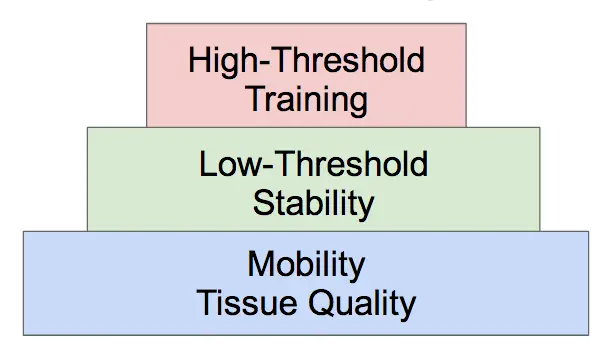
Start at the bottom of the pyramid and work your way up
Bottom Line
There’s already enough to think about when selecting exercises (pathology, movement pattern, biomechanics, kinesiology, anatomy, etc.). And it sucks to add more to the list. But if your patient is using a dysfunctional high-threshold strategy the rest of the list doesn’t matter. By keeping tabs on the threshold strategy your exercise prescription will only be more effective.
References
Gray Cook – Movement
Charlie Weingroff – Training=Rehab, Rehab=Training
—
The main reason I do this blog is to share knowledge and to help people become better clinicians/coaches. I want our profession to grow and for our patients to have better outcomes. Regardless of your specific title (PT, Chiro, Trainer, Coach, etc.), we all have the same goal of trying to empower people to fix their problems through movement. I hope the content of this website helps you in doing so.
If you enjoyed it and found it helpful, please share it with your peers. And if you are feeling generous, please make a donation to help me run this website. Any amount you can afford is greatly appreciated.



Thank you thank you for an excellent article…will share with my staff for sure! So, I am confused by:”The Threshold-Breathing-Continuum: Parasympathetic diaphragm breathing is used in low-threshold strategies. Breath holding and valsalva is used in high-threshold strategies.” I believe you differentiate between functional and dysfunctional high-threshold strategies. Is valsalva ever a functional stategy? I know it is taught a lot in weight lifting. Non-weightlifting-Pilates-instructor is curious. Thanks!
Great Question Margy!
A quick distinction here just to avoid confusion. The valsalva is the act of forced expiration against closed airways. Valsalva is never a functional strategy.
An important part of the breathing-stability concept is that there should be an inhale prior to bracing. This inhale increases the IAP which is the key to passive pressurized stability. Weightlifters should employ an inhale, pause, and brace prior to the lift.
Back to your question…
Short Answer: No
Long Answer: No for valsalva, but yes for inhale & brace
The act of holding your breath (after inhalation) and bracing can be functional if the task is a high-load/velocity/force. A powerlifter better hold their breath and brace coming out of the bottom of the squat or they will lose some valuable stability.
This can also be functional when your sedentary business man is going to pick up his heavy luggage. If he lifts with the right mechanics, holds his breath for a second as he initiates the lift, and then exhales he will maximize his stability and decrease his risk of injury. Lifting with all of his air expired would rob him of this pressurized stability.
For other activities like Pilates and yoga it depends on the task. You don’t want someone in Warrior I or someone doing 100s with full bracing and breath holding. However, for high-load/velocity/force tasks it may be appropriate. For example, the jump to chaturanga would require a split second of holding the breath during the transition. I’m not an expert on Pilates, but I would think for the most part you would not want a full inhale/breath holding moment. If someone is in this high-threshold breath holding state it may be a sign that the exercise is too advanced for them.
Thanks for an excellent answer! Learned a lot. I will be following your blog for sure!
[…] for strength training. Aaron Swanson has a great blog on low versus high threshold strategies here – his explanations are listed […]